MAST CELL TUMORS
Michelle LaRue, DVM, MS
Diplomate, ACVIM, Oncology
Mast cell tumor (MCT) is the most common skin cancer of dogs, though can less commonly originate in other locations, such as the spleen, liver, and bone marrow. It involves an overgrowth of mast cells, which are part of the body’s immune system. They can be triggered to release several chemicals that are important in the body’s defenses. When they become cancerous, however, they can release large amounts of these chemicals inappropriately, causing irritation, gastrointestinal upset, and other side effects. Like many other cancers, these tumors can metastasize to other skin sites, lymph nodes, and distant organs (especially spleen or liver). These tumors are assigned various grades that correspond to their aggressiveness and thus the likelihood that they will invade other tissues.
Depending on the grade of the tumor, we may recommend initial staging tests (lymph node aspirate, chest x-rays, and abdominal ultrasound) to look for any evidence of cancer spread. Mast cell tumors generally do not spread to the lungs, though x-rays would be recommended to evaluate the heart and lungs prior to a second surgery and overall health. An abdominal ultrasound can be performed to look for any evidence of cancer spread to the liver or spleen, which are one of the more common places for mast cell tumors to spread. Samples need to be taken from the liver or spleen to determine if there is cancer present or not.
Treatment Options:
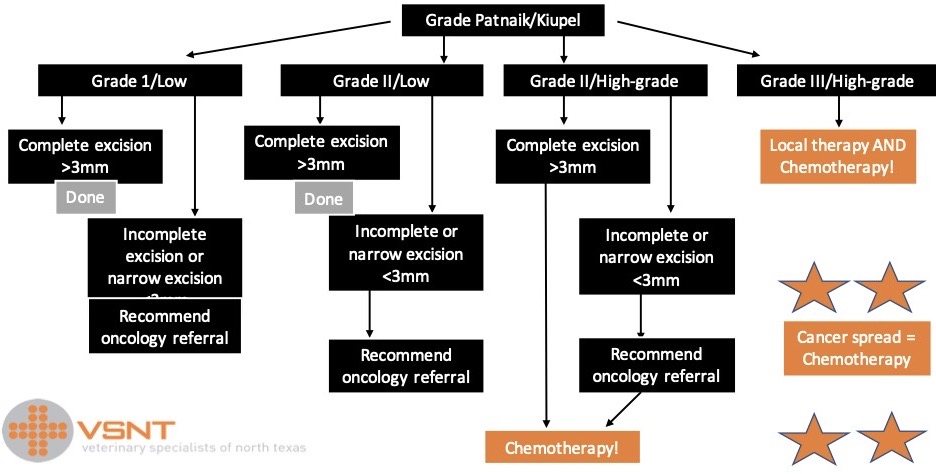
1) Surgery is the cornerstone of treatment for most mast cell tumors. Biopsy results allow us to determine grade and surgical margins. With this information we are then able to best decide on further treatment if needed.
When tumor cells are left behind after surgery, or margins are extremely close, we typically recommend some form of follow-up treatment, whether a second surgery, radiation therapy, chemotherapy, or some combination thereof.
2) Radiation Therapy – When a second surgery is not feasible or there is a large tumor that cannot be removed, the next best option for local control is radiation therapy.
3) Chemotherapy – Traditional chemotherapy may be used after surgery if margins are not complete, or with tumors that have an increased likelihood of metastasizing, such as grade III MCTs. As we discussed, dogs tend to tolerate chemotherapy better than humans, with the most common side effects being gastrointestinal upset and suppression of the immune system. Commonly used for treatment of MCTs are vinblastine, CCNU (lomustine), Palladia, and steroids. We check a complete blood count (CBC) before each treatment to make sure it is safe to give chemotherapy. With more aggressive mast cell tumors, we also recommend rechecking an abdominal ultrasound at the beginning, midpoint, and again when the protocol is finished to monitor for any evidence of cancer spread. Other chemotherapy may also be discussed depending on the grade of the tumor.
We also briefly discussed the use of prednisone (steroids) in mast cell tumors. The side effects include increased thirst, increased urination, increased appetite, and panting. These effects may improve or resolve as we decrease the dosage of prednisone used.
4) Electrochemotherapy – This treatment can be used to control local cancer regrowth. It requires anesthesia to injection chemotherapy at the site and/or IV. An electrical pulse opens the cancer cells to absorb the chemotherapy treatment. This allows more concentrated/local treatment of remaining tumor cells.
5) Other recommended medication – Also, with higher grade mast cell tumors or presence of metastasis, there is a concern that your dog may develop a stomach ulcer due to a release of histamine, which can occur secondary to his/her mast cell tumor. We therefore would like to start them on a gastric protectant (whether Prilosec (omeprazole) or Pepcid(famotidine)) to help any potential ulcers heal.